
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist. The swelling in lymphedema is caused by an abnormal accumulation of protein and water molecules in the tissue and results from the inability of the lymphatic system to perform one of its basic functions, the removal of water and protein from the body tissues. This insufficiency can be caused by developmental abnormalities of the lymphatic system (primary lymphedema), or damage to the lymphatic system, such as the removal or radiation of lymph nodes in cancer surgery, or infection of the lymphatic system (secondary lymphedema).
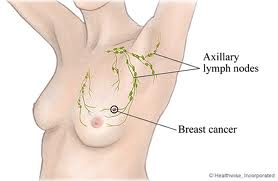 The highest incidence of secondary lymphedema in the United States is observed following surgery and radiation for malignancies, particularly among those individuals affected by breast cancer. Generally, it can be said that one out of eight women in the U.S. will develop breast cancer during the course of their lives. At the present time, almost 227,000 new cases of breast cancer in females and 2200 in males are estimated in the United States annually (1).
The highest incidence of secondary lymphedema in the United States is observed following surgery and radiation for malignancies, particularly among those individuals affected by breast cancer. Generally, it can be said that one out of eight women in the U.S. will develop breast cancer during the course of their lives. At the present time, almost 227,000 new cases of breast cancer in females and 2200 in males are estimated in the United States annually (1).
To reduce the swelling, it is necessary to re-route the stagnated lymph flow around the blocked area(s) into more centrally located healthy lymph vessels. This goal is achieved by a combination of different treatment modalities, all of which are integral components of Complete Decongestive Therapy (CDT), the internationally recognized “gold standard” (2,3) treatment system for the vast majority of patients affected by lymphedema. CDT components include:
 Manual Lymph Drainage (MLD),
Manual Lymph Drainage (MLD),
Decongestive and breathing exercises and
CDT is performed in two phases; in the first phase, also known as the intensive phase, treatments are administered by trained lymphedema therapists on a daily basis until the affected body part is decongested.
The results of measurements on the affected body part (taken by the therapist) determine the end of the first phase of CDT; once measurements approach a plateau, the end of phase one is reached, and the patient progresses seamlessly into phase two of CDT. Phase two, also known as the self-management phase, is an ongoing and individualized part of CDT, in which the patient assumes responsibility for maintaining and improving the treatment results achieved in phase one.
During the intensive phase, the patients are instructed in the individual components of self-management, which include a skin care regimen, home exercises, self-manual lymph drainage and the application of compression garments for daytime use.
Backed by long standing experience, CDT has shown to be safe and effective as the standard therapy for lymphedema. It is listed on the web sites of the American Cancer Society, the National Cancer Institute, the International Society of Lymphology and the National Lymphedema Network as the main component in the treatment and management of primary and secondary lymphedema.
Applied correctly by a skilled and certified lymphedema therapist, CDT shows excellent long-term results in both primary and secondary lymphedema.
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Join Lymphedema Guru, a Facebook page solely dedicated to inform about all things related to lymphedema – news, support groups, treatment centers, and much more
(1) National Cancer Institute http://cancer.gov/cancertopics/types/breast
(2) Position Statement of the National Lymphedema Network on the diagnosis and treatment of lymphedema 2011_NLN_Position-Statement-of-NLN.pdf
(3) Textbook of Palliative Nursing http://books.google.com/books?id=0C6FT028S4sC&pg=PA292&lpg=PA292&dq=gold+standard+for+lymphedema+treatment&source=bl&ots=tNeU4KFYmh&sig=3IhCkM0UOiOanV3wVXg78qRbV0I&hl=en&sa=X&ei=_C8aU-qeN8-DkQfbjIHIBg&ved=0CDUQ6AEwAg#v=onepage&q=gold%20standard%20for%20lymphedema%20treatment&f=false


I have a Lymphedema pump now which is helping to get the edema out of my legs. I can not wear the compression stockings as they cut the circulation out of my ankles and underneath knees…The doctor recommended the pump.
there’s a lot of self teaching/therapy going on because of the expense of treatment and continuing limited access through healthcare insurers. i have to pay cash for my garment so instead of change up every 3-6 months, it’s more like every 2-3 years which defeats the whole purpose. what’s to do? thanks.
I have had left arm lymphedema for five years due to breast cancer surgery. My exercise of choice is swimming. I would appreciate seeing specific water exercises to help, not harm, my condition. I am always afraid of exercising too much or not enough.
Thank you.
This article may be of interest to you: https://www.lymphedemablog.com/2011/01/20/the-benefit-of-aquatic-exercise-for-lymphedema/
I am familiar with the Voder Method. Which method of practice do you refer to?
We are always referring to the Vodder method of Manual Lymph Drainage
I have lipedema of both legs, wear compression garments and do lymph drainage massage daily using a Flexi Touch machine provided by my insurance carrier. Do you have any other advice for me?
Dear Mary: the main goal in the management of lipedema is to prevent increase in swelling. You are doing the right things to do that.
Since having sinus surgery in February I have had submandibular swelling and lower eye-lid bags. Some improvement has occurred. The swelling is greater when lying down at night and diminishes when up during the day. The eye-bags are less variable. My surgeon says persistent swelling in these areas wouldn’t be related to sinus surgery, however, it developed right after it. Your opinion/advice would be appreciated. Thank you, Steven
Steven: It is irrelevant if the sinus surgery is related to persistent swelling or not. It is important to take care of the swelling as soon as possible. Here is a link to an article you may find interesting: https://www.lymphedemablog.com/2012/05/11/secondary-lymphedema-of-the-head-and-neck/
I would like some information on how to treat cording after a mastectomy. This cording runs from the armpit down across the chest around the ribs into the hip and towards the navel.
Any info greatly appreciated.
Regards Bronwyn
Here is a link to an article on the subject: https://www.lymphedemablog.com/2011/04/28/axillary-web-syndrome/
Hello, I can’t find where to leave a question on the website. I’m in my 50’s have primary lymphodema in both legs and chronic venous insufficiency. I have now been diagnosed with moderate arthritis in both knees. I have been wrapping my knees with compression bandages at night to keep the swelling down but have a fair amount of pain. The doctor wants me to consider cortisone shots, my physio considers it a last resort. I’m wondering if a tens unit would be beneficial for knee pain or if it would have an adverse affect on my lymphodema. I was looking at the dr ho circulation promoter so my husband could use it too. Are there any therapies you could recommend?