
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist. 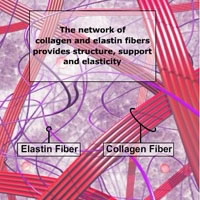 It is important to understand that the elastic fibers in the tissues affected by lymphedema are damaged. These fibers lose their elasticity and tend to harden, which is particularly the case in untreated lymphedema present over a long period of time and progressed stages of lymphedema.
It is important to understand that the elastic fibers in the tissues affected by lymphedema are damaged. These fibers lose their elasticity and tend to harden, which is particularly the case in untreated lymphedema present over a long period of time and progressed stages of lymphedema.
Although the swelling in lymphedema may be reduced to a normal or near normal size during treatments, the damage to the lymphatic system, which caused the onset of lymphedema, is permanent and the skin elasticity in the tissues affected by lymphedema may never be regained to prior levels.
Contrary to edema, a low-protein swelling, lymphedema is a disease rather than a symptom and its underlying cause, the insufficiency of parts of the lymphatic system cannot be reversed.
 Lymphedema results from the inability of the lymphatic system to perform one of its basic functions, the removal of water and protein from the tissues of a portion of the body. This insufficiency can be caused by developmental abnormalities of the lymphatic system (primary lymphedema), or damage to the lymphatic system such as the removal or radiation of lymph nodes in cancer surgery, or infection of the lymphatic system (secondary lymphedema).
Lymphedema results from the inability of the lymphatic system to perform one of its basic functions, the removal of water and protein from the tissues of a portion of the body. This insufficiency can be caused by developmental abnormalities of the lymphatic system (primary lymphedema), or damage to the lymphatic system such as the removal or radiation of lymph nodes in cancer surgery, or infection of the lymphatic system (secondary lymphedema).
The accumulation of protein and water in the tissues may be gradual in some patients and sudden in others, the result is always a high-protein edema.
Lymphedema does not dissipate by itself and continues to progress without adequate treatment.
The goal of lymphedema management is to reduce the lymphedematous swelling to a normal or near normal size utilizing remaining healthy lymph vessels and other lymphatic pathways. Once the lymphedema is decongested, the secondary goal is to maintain the reduction and to prevent the re-accumulation of lymph fluid.
These goals can be achieved with the internationally recognized “gold standard” of lymphedema treatment known as Complete (or Combined) Decongestive Therapy (CDT). CDT is a combination of the following treatment modalities:
Manual lymph drainage (MLD), skin care, decongestive exercises and compression therapy.
 Compression therapy in lymphedema management is provided either via bandages, compression garments or alternative compression devices (depending on the stage of treatment).
Compression therapy in lymphedema management is provided either via bandages, compression garments or alternative compression devices (depending on the stage of treatment).
Compression bandages and garments by themselves will not reduce existing swelling and must therefore not be worn on an untreated, swollen extremity.
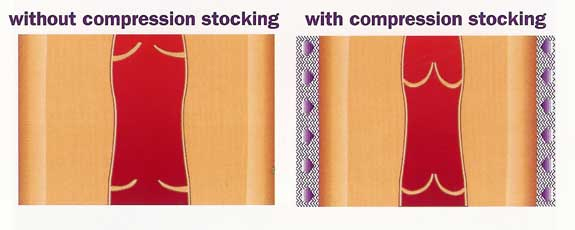
 Individuals affected by lymphedema graduate from padded short-stretch bandages, which are applied by the lymphedema therapist in the intensive phase of CDT to elastic compression garments only when the affected extremity is decongested. To assist in the movement of fluids back to the heart, a pressure gradient between the lower (higher pressure) and the upper part (lower pressure) of the extremity is provided with bandages and garments.
Individuals affected by lymphedema graduate from padded short-stretch bandages, which are applied by the lymphedema therapist in the intensive phase of CDT to elastic compression garments only when the affected extremity is decongested. To assist in the movement of fluids back to the heart, a pressure gradient between the lower (higher pressure) and the upper part (lower pressure) of the extremity is provided with bandages and garments.
Even after successful treatment, the body part affected by lymphedema is at permanent risk for re-accumulation of fluid and most individuals affected by lymphedema are aware of the fact that this condition requires life-long care.
Without the benefits of external compression successful long-term management of lymphedema would be very difficult and in most cases impossible.
So why is compression therapy an essential component in lymphedema management?
As explained, the elastic fibers in lymphedema are damaged and thus unable to provide sufficient resistance to the build-up of fluid in the interstitial tissue spaces. The application of external compression provides the necessary support for those tissues that lost elasticity and compensates for the elastic insufficiency by increasing the tissue pressure.
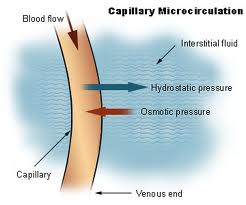 The tissue pressure plays an essential role in the exchange of fluids between the blood capillaries and the tissue. The increased tissue pressure provided by external compression reduces the amount of fluid leaving the blood capillaries into the tissues and increases the return of tissue fluids back into the blood and lymph capillaries, thus reducing the amount of fluid in the tissues.
The tissue pressure plays an essential role in the exchange of fluids between the blood capillaries and the tissue. The increased tissue pressure provided by external compression reduces the amount of fluid leaving the blood capillaries into the tissues and increases the return of tissue fluids back into the blood and lymph capillaries, thus reducing the amount of fluid in the tissues.
 External compression also increases venous and lymphatic return by improving the function of the valves in these vessels. Another important factor for sufficient return of venous and lymphatic fluids back into the blood stream is the movement of skeletal musculature and joints during activity. Together with other supporting mechanisms the muscle and joint pump activity propels these fluids back to the heart and ensures uninterrupted circulation.
External compression also increases venous and lymphatic return by improving the function of the valves in these vessels. Another important factor for sufficient return of venous and lymphatic fluids back into the blood stream is the movement of skeletal musculature and joints during activity. Together with other supporting mechanisms the muscle and joint pump activity propels these fluids back to the heart and ensures uninterrupted circulation.
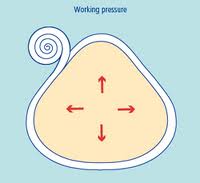 External compression provides a counter force to the working musculature, known as working pressure, thus improving its efficiency.
External compression provides a counter force to the working musculature, known as working pressure, thus improving its efficiency.
These effects help to prevent re-accumulation of fluids which were evacuated during intensive CDT treatments and conserve the results achieved during MLD.
Another positive impact of compression therapy is the softening of hardened connective tissue often present in lymphedema, especially if external compression therapy is combined with special foam materials.
More articles on this subject:
How to Care for Compression Garments
Click here for a PDF Version of this Article
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Join Lymphedema Guru, a Facebook page solely dedicated to inform about all things related to lymphedema – news, support groups, treatment centers, and much more

