
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist.
“After a day of sitting in the office my ankles are swollen.”
“During the last several months of my pregnancy, my legs practically doubled in size”
“My fingers and hand frequently get puffy following a long hike”
“My arm started swelling after I had surgery for my breast cancer”
“Following the removal of a malignant lesion on my thigh, my leg started to get bigger”
“When I got stung by a bee on my cheek, I had a big swelling covering the entire side of my face”
Does any of this sound familiar? In some of these cases the term “swelling” can be interchangeably used with edema, in other cases the swelling must be considered as lymphedema. While the initial causes for the formation of the swelling in the above instances are different, all involve the accumulation of fluid in the soft tissues of the skin due to an insufficiency of the lymphatic system.
A physician with knowledge of lymphedema is able to easily establish the diagnosis of lymphedema by taking the patients medical history and performing a physical examination. This includes measuring the circumference of the affected arms or legs to determine the severity of fluid buildup in affected limbs. The physician determines whether symptoms, such as swelling in the arms or legs, might be caused by other conditions, including blood clots, or cardiac insufficiencies, which are treated differently. To further establish the diagnosis, certain imaging tests may be performed in order to conclude the exact cause of the fluid buildup in the tissues.
These tests may include:
- Lymphscintiography (most commonly performed and considered to be the gold standard)
- Bioimpedance Spectroscopy (BIS)
- ICG Lymphography (Indocyanine Green), sometimes referred to as Fluoroscopy
- MRI
- CT
- Indirect Lymphography (not commonly performed in the US)
- others
You can also perform a self-check for Lymphedema before you make an appointment with a physician – take a personal assessment by answering the following questions:
- Is the swelling limited to one arm or leg?
- Did you have surgery or radiation prior to the onset of the swelling?
- Did you have an injury on your affected body part?
- Is the back of the hand/foot included in the swelling?
- Are the natural skin folds (elbow/knee, ankle/wrist) on your extremity deepened?
If the answer to some or all the above questions is “yes”, lymphedema may be present.
You can also perform the “Stemmer” Test by trying to lift a skin fold on the back of the second toe or middle finger.
If you are able to gently pinch and lift the skin fold, the Stemmer Sign is negative. If it is not possible to gently pinch and lift the fold, this may be an indication of tissue build-up as a result of protein accumulation in these tissues. In this case, the Stemmer Sign is positive and serves as an indication that lymphedema may be present. Please see below to learn about the treatment of lymphedema.
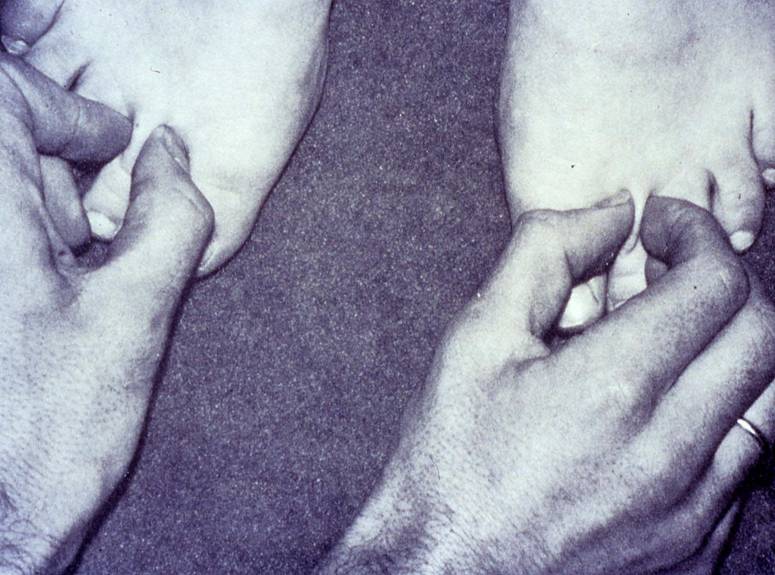
Stemmer sign positive on left (right leg)
Click here to view a video explaining the physicians diagnosis of lymphedema
The question is – when is a swelling considered edema, and when is it lymphedema?
In order to understand the differences, it is important to consider that a large portion of the human body consists of water. According to Guyton’s  Textbook of Medical Physiology, the water content of an average weight male is about 60%, in a female about 55%; in a male weighing 160 pounds, this amounts to approximately 40 liters (about 10.5 gallons) of water. About two thirds of the water resides inside the body’s cells in the intracellular fluid compartment, one third is located outside the cells in the extracellular compartment. Of the fluid residing outside the cells, one fifth is located inside blood vessels as intravascular fluid. The remaining fluid (approximately 10.5 liters) is distributed in the interstitial tissue between the cells (interstitial fluid).
Textbook of Medical Physiology, the water content of an average weight male is about 60%, in a female about 55%; in a male weighing 160 pounds, this amounts to approximately 40 liters (about 10.5 gallons) of water. About two thirds of the water resides inside the body’s cells in the intracellular fluid compartment, one third is located outside the cells in the extracellular compartment. Of the fluid residing outside the cells, one fifth is located inside blood vessels as intravascular fluid. The remaining fluid (approximately 10.5 liters) is distributed in the interstitial tissue between the cells (interstitial fluid).
 Fluids, gases (oxygen and carbon dioxide), nutrients and waste products are constantly exchanged between the blood and the interstitial tissue. The primary sites of this exchange are the blood capillaries, which are the smallest blood vessels and part of the body’s microcirculation. Blood capillaries have very thin walls, consisting of only one layer of cells. Gaps between these cells enable the exchange of these substances from the blood capillaries into the tissues and back. The water located in the interstitial tissue spaces is fluid that has leaked out of blood capillaries.
Fluids, gases (oxygen and carbon dioxide), nutrients and waste products are constantly exchanged between the blood and the interstitial tissue. The primary sites of this exchange are the blood capillaries, which are the smallest blood vessels and part of the body’s microcirculation. Blood capillaries have very thin walls, consisting of only one layer of cells. Gaps between these cells enable the exchange of these substances from the blood capillaries into the tissues and back. The water located in the interstitial tissue spaces is fluid that has leaked out of blood capillaries.
Edema occurs when excess levels of interstitial fluid accumulate, i.e., either too much water leaves the blood capillaries, or the water located in the tissues is not reabsorbed efficiently enough back into the blood capillaries. Edema may affect the entire body (anasarca, or generalized edema), or only certain parts of the body (localized edema).
In order to understand any swelling, the various factors and components involved in moving fluids throughout the body, and in and out of blood vessels need to be considered. The main components involved in this process are the cardiovascular system (heart and blood vessels) and the lymphatic system.
The cardiovascular system consists of an elaborate network designed to deliver oxygen and nutrients to body organs and to remove waste products  of metabolism from the tissues. Blood that has been oxygenated in the lungs is pumped out of the heart through the aorta, the largest artery in the body. The aorta arches upward from the left ventricle of the heart to the upper chest, and then travels down towards the abdomen forming the main trunk of the arterial circulation. The aorta then branches off into numerous smaller arteries, which deliver oxygen-rich blood to the various body systems. These arteries further subdivide into smaller vessels, and ultimately into blood capillaries, which consist of an arterial and a venous loop. The exchange of fluids, gases, nutrients and waste products between blood and tissue occurs across their walls.
of metabolism from the tissues. Blood that has been oxygenated in the lungs is pumped out of the heart through the aorta, the largest artery in the body. The aorta arches upward from the left ventricle of the heart to the upper chest, and then travels down towards the abdomen forming the main trunk of the arterial circulation. The aorta then branches off into numerous smaller arteries, which deliver oxygen-rich blood to the various body systems. These arteries further subdivide into smaller vessels, and ultimately into blood capillaries, which consist of an arterial and a venous loop. The exchange of fluids, gases, nutrients and waste products between blood and tissue occurs across their walls.
On its way back to the heart, the venous blood passes through progressively larger veins and ultimately connects with the heart. A large part of the waste products is extracted from the blood as it flows through the kidneys.
The lymphatic system consists of lymph nodes and a network of channels in the body that carry lymph fluid, which is a colorless fluid containing mainly  water, protein and white blood cells. The water content in the lymph fluid is comprised by a fraction of the fluid, which leaves the blood capillaries, but is not reabsorbed back into the blood capillaries. The lymphatic system runs parallel to the blood circulatory system and represents an accessory route for fluid to flow from the tissue spaces back to the bloodstream. The lymph fluid is returned to the blood circulation via larger lymphatic vessels (lymphatic trunks) and amounts to approximately 2-3 liters per day. Unlike the circulatory system, in which the heart acts as a pump to circulate blood, the lymphatic system does not have a pump to circulate lymph fluid. Instead, larger lymph vessels contain small muscles (lymph angions) within their walls, which contract consecutive sections of the lymph vessels to facilitate the movement of lymph through its vessels via a peristaltic effect.
water, protein and white blood cells. The water content in the lymph fluid is comprised by a fraction of the fluid, which leaves the blood capillaries, but is not reabsorbed back into the blood capillaries. The lymphatic system runs parallel to the blood circulatory system and represents an accessory route for fluid to flow from the tissue spaces back to the bloodstream. The lymph fluid is returned to the blood circulation via larger lymphatic vessels (lymphatic trunks) and amounts to approximately 2-3 liters per day. Unlike the circulatory system, in which the heart acts as a pump to circulate blood, the lymphatic system does not have a pump to circulate lymph fluid. Instead, larger lymph vessels contain small muscles (lymph angions) within their walls, which contract consecutive sections of the lymph vessels to facilitate the movement of lymph through its vessels via a peristaltic effect.
Under normal conditions the body thrives to maintain a balance of fluid in the tissues by ensuring that about the same amount of water entering the body also leaves it. However, a number of factors can upset the fluid balance in the body, which may cause the onset of edema or lymphedema.
Edema
Rather than a disease in itself, edema is a symptom that can be caused by a number of conditions, including:
- Congestive heart failure (CHF),
- Chronic venous insufficiency (CVI),
- Immobility (prolonged standing or sitting, paralysis)
- Pregnancy, or
- Pressure from tight jewelry, tight bandages or compression garments
In all these cases the accumulation of fluid in the interstitial tissues is caused by insufficient return of venous blood, or venous pooling. The high volume of blood and the consequent increase in hydrostatic pressure inside the veins and blood capillaries makes it difficult for fluid to move from the tissues back into the vessels. While the lymphatic system tries to correct this imbalance by working harder, the elevated levels of tissue fluid is too high for the lymph vessels to compensate.
Edema may also be caused by change in the concentration of serum proteins (hypoproteinemia). Proteins in the blood have the ability to retain some water and salts within the blood, and a lower level of proteins may affect the movement of fluid in and out of blood capillaries causing excess levels of water to accumulate in the tissues. A loss of serum proteins may be caused by kidney, liver or thyroid diseases, malnutrition, excessive bleeding, chronic draining wounds and excessive burns.
Inflammatory reactions caused by traumatic events and arthritis are also a common cause for the onset of edema.
 Edema is a visible and palpable accumulation of excess levels of fluid within the tissues. Gentle, steady pressure with a thumb on the edematous tissues produces a temporary indentation (pitting edema). Edema can be a transitory or permanent symptom and its treatment focuses on the correction of the underlying condition; if this condition can be resolved the edema dissipates. If the underlying cause can’t be corrected, edema may be treated by elevation of the affected body part, wearing compression garments, the administration of diuretics, or dietary changes focusing on a low salt intake.
Edema is a visible and palpable accumulation of excess levels of fluid within the tissues. Gentle, steady pressure with a thumb on the edematous tissues produces a temporary indentation (pitting edema). Edema can be a transitory or permanent symptom and its treatment focuses on the correction of the underlying condition; if this condition can be resolved the edema dissipates. If the underlying cause can’t be corrected, edema may be treated by elevation of the affected body part, wearing compression garments, the administration of diuretics, or dietary changes focusing on a low salt intake.
Lymphedema
Lymphedema results from the inability of the lymphatic system to perform one of its basic functions, the removal of water and protein from the tissues of a certain portion of the body. This insufficiency can be caused by  developmental abnormalities of the lymphatic system (primary lymphedema), or damage to the lymphatic system such as the removal or radiation of lymph nodes in cancer surgery, or infection of the lymphatic system (secondary lymphedema). Lymphedema can present in the extremities, head and neck, breast and trunk, or external genitalia. The accumulation of protein and water in the tissues may be gradual in some patients and sudden in others, the result is always a high-protein edema. The high protein content in lymphedema can lead to secondary complications, such as hardening of the tissues over time, infections and increase in volume, especially in untreated or mistreated lymphedema.
developmental abnormalities of the lymphatic system (primary lymphedema), or damage to the lymphatic system such as the removal or radiation of lymph nodes in cancer surgery, or infection of the lymphatic system (secondary lymphedema). Lymphedema can present in the extremities, head and neck, breast and trunk, or external genitalia. The accumulation of protein and water in the tissues may be gradual in some patients and sudden in others, the result is always a high-protein edema. The high protein content in lymphedema can lead to secondary complications, such as hardening of the tissues over time, infections and increase in volume, especially in untreated or mistreated lymphedema.
Contrary to edema, a low-protein swelling, lymphedema is a disease rather than a symptom and its underlying cause, the insufficiency of parts of the lymphatic system cannot be reversed. Lymphedema does not dissipate by itself and continues to progress without adequate treatment.
Treatment of Lymphedema
The goal of lymphedema management is to reduce the lymphedematous swelling to a normal or near normal size utilizing remaining healthy lymph vessels and other lymphatic pathways. Once the lymphedema is decongested, the secondary goal is to maintain the reduction and to prevent the reaccumulation of lymph fluid. These goals can be achieved with the internationally recognized “gold standard” of lymphedema treatment known as Complete (or Combined) Decongestive Therapy (CDT). CDT is recognized as the therapy of choice for lymphedema by the International Society of Lymphology (ISL), the National Lymphedema Network (NLN), the Lymphology Association of North America (LANA), the American Lymphedema Framework Project (ALFP), and the North American Lymphedema Education Association (NALEA).
CDT is a combination of manual lymph drainage (MLD), a gentle manual treatment technique designed to reroute stagnated lymph fluid, skin care, compression therapy (short-stretch bandages and compression garments), and decongestive exercises.
CDT should only be performed by properly trained therapists. Lymphedema therapists can be physical therapists and their assistants, occupational therapists and their assistants, physicians, nurses, chiropractors or massage therapists who have undergone specialized training in Complete Decongestive Therapy. Several schools in the United States educate and certify therapists in proper lymphedema management; these schools meet the training standards outlined by the Lymphology Association of North America (LANA).
Pharmaceutical options in the treatment of lymphedema are limited to antibiotics, which are used to prevent and treat infections commonly associated with lymphedema. Diuretics are generally harmful and may contribute to the worsening of lymphedema related symptoms if used long-term.
Intermittent pneumatic compression devices (IPC) may be indicated in suitable cases, but should always be used in combination with CDT and never as a sole mode of treatment.
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Join Lymphedema Guru, a Facebook page solely dedicated to inform about all things related to lymphedema – news, support groups, treatment centers, and much more

