
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist.
I would like to thank Frank Aviles, Jr., PT, CWS, WCC, FACCWS, CLT, MLD/CDT and Wound Care Instructor, a well-known specialist on the topic of open and weeping wounds associated with edema and lymphedema, to provide this very informative and important article.
Chronic Wound Care: Reading The Weep (by Frank Aviles)
Management of excessive lower extremity drainage is often difficult. Patients may have to resort to holding a bucket to collect the drainage from their legs, the need to change their dressing and/or clothing may seem continuous. Excessive drainage can damage skin when prolonged contact is experienced and create an environment for infection, slow healing, and decreased quality of life. Then there’s the frustration of the costs of supplies and insurance concomitantly troubling patients and providers.
In this article I would like to discuss what edema is, possible causes, and what happens when not addressed properly such as typically encountered weeping legs. I will refer to the traditional Starling principle but be aware that the revised Starling principle indicates an increase role for the lymphatic and not the venous system in removing drainage.
When dealing with “weepy” or “leaky” legs, it is imperative to understand and treat the underlying cause. Peeling the layers of this problem can ensure proper treatment to decrease the amount of drainage experienced. Swelling can be caused by various conditions and the treatment must be directed at the cause. It is not uncommon for people to seek medical help for their extremity swelling and for providers to quickly order the diuretic “water pill” to resolve the problem. Is this the right thing to do for our swollen patients? For certain conditions such as heart failure or liver disease, providers may prescribe diuretics to reduce fluid in the body to lessen symptoms such as shortness of breath and swelling in the extremities or abdomen. But if the cause is related to conditions such as chronic venous insufficiency or lymphedema, then the culprit of swelling is not addressed, making the diuretic a treatment that is prolonging the inevitable.
When it comes to chronic wound care, a non-healing wound is often a symptom of a disease, and proper recognition should lead to proper treatment.
After an injury or a surgical procedure, swelling is considered to be part of the normal healing process. Ultimately, the “TRUE” cause of the swelling will determine how it will be treated. Prolonged and unmanaged swelling can trigger inflammatory–related changes in the tissue progressing to skin infection, wounds, and a weeping extremity. Understanding the cause of the swelling along with the healing process will lead to selecting proper interventions.
The healing cascade is an overlapping series of events that must occur in a forward direction, allowing the body to heal. It begins with the inflammatory phase, when cellular events take place in response to an acute injury. Characteristics for this phase include redness, warmth, and swelling that may last up to 4 days. The second phase, the proliferative phase, includes new blood vessels beginning (angiogenesis), and collagen being laid down to form the foundation for cells during the repair process. The final phase, the maturation or remodeling phase, is where the new “scar” tissue matures, lasting up to 2 years. When the series of events do not progress in a forward direction, a wound will become chronic and remain inflammatory. Identifying the contributing factors, that is maintaining the tissue in the chronic and inflammatory state will be essential.
WHAT IS EDEMA?
Edema is the collection of fluid in the interstitial space due to a systemic or local condition. Understanding its etiology will drive its treatment. Systemically, when the body fails to maintain a state of equilibrium, swelling can develop and be caused by various systems. Let’s examine conditions that can create swelling:
- The cardiac system – congestive heart failure, left–side heart failure, vein valvular incompetence, lymphatic involvement, hypoprotenimia (low protein concentration in the blood), or poor ejection fraction;
- The musculo-skeletal system with a poor calf pump mechanism;
- The respiratory system with pulmonary edema, COPD or emphysema;
- The urinary system with kidney failure;
- Liver failure.
Locally, edema can be best explained by understanding what occurs at the capillary level. The capillary is responsible for the exchange of oxygen, nutrients, and waste products as it sustains cell life. The anatomy of the capillary consists of an arterial side, in which the volume is controlled by a smooth muscle – the precapillary sphincter, a venous side, and a few lymphatic structures. As blood enters the arterial side of the capillary, oxygen and nutrients are delivered to the cells while water leaves the system based on pressure differences. The venous side will remove water and waste products from this space back into the vascular system. The corresponding lymphatic vessels at the capillary will remove waste products that are not able to be removed by the venous system, as its too large. A small percentage of water will also be removed by the lymphatic system. When this delicate balance is disturbed at the capillary level, edema (or protein rich edema, i.e. lymphedema) will occur. Unlike a disturbance on the arterial side, the venous and/or lymphatic system disturbance will create an increase in interstitial fluid, causing an edematous response or swelling. Swelling can disturb the healing process because it increases the distance for the delivery of oxygen and nutrients, as well as the removal of waste products. This can be described as increasing the diffusion distance. Treatment is aimed at determining the cause of the swelling, and if it’s not of systemic nature, the aim should be to decrease diffusion distance by lower extremity elevation and appropriate compression.
PROLONGED EDEMA
Persistent swelling without adequate treatment can lead to chronic wounds. After a wounding event, the body will go through the repair process or through the phases of healing. When the repair process stalls in the inflammatory phase, as in the example of chronic wounds or edematous extremities, the wound and skin will undergo certain changes due to this inflammatory response and state. Prolonged swelling will induce this inflammatory condition, which will affect the tissue over time. The texture of the skin will become hard (fibrotic) and cause the skin to have a red hue, which may complicate treatment. Fibrosis is the end result of chronic inflammation reactions.
Additionally, legs will start to weep as increased fluid in the interstitial space looks to escape as it’s not being reabsorbed into the system. If the patient has a venous–related problem, prolonged infection, or even a faulty calf-pump mechanism, we may end up with phlebo-lymphedema due to lymphatic involvement on top of the venous condition. When excess protein remains in the tissue for an extended duration, an inflammatory reaction will occur. This high protein–rich fluid in the interstitial space will lead to increased weepiness as protein molecules have a tendency to “hold” water molecules and compression alone will not push this fluid back through the normal process.
“THAT WEEPY LEG”

Leg before CDT and compression. Weeping is visible
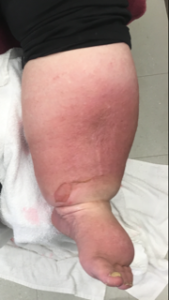
Leg after CDT and compression
When considering weeping legs, multiple conditions come to mind – a systemic condition, such as hypoprotenemia, cardiac issues, liver failure, or chronic progressive untreated swelling. The treatment for the systemic condition is aimed at addressing the culprit, whereas the latter requires adequate compression. At the capillary level on the arterial side, there is a balance between water leaving the circulatory system into the interstitial space known as filtration while on the venous side most of the water gets reabsorbed into the circulatory system, a process known as reabsorption. When filtration increases or reabsorption decreases an extra accumulation of fluid will be collected in the interstitial space.
For patients with chronic venous insufficiency (CVI) or a faulty venous system, compression is typically utilized to decrease filtration of extra interstitial fluid. When compression is appropriately applied, weepiness decreases. If the patient has lymphatic involvement, treatment will be aimed at appropriate compression along with other strategies to remove the excessive protein found in the interstitial space. Compression and diuretics alone will not be effective at this stage. The “gold standard” treatment when lymphedema is present will be complete decongestive therapy (CDT). CDT has four components that include skin care, manual lymphatic drainage, compression, and exercise. Compression initially will take the form of short–stretch bandages and progress to compression garments. The compression will progress from a form of treatment to one that is applied by the patient after adequate girth reduction is achieved. These conditions, such as CVI and lymphedema, will require lifelong management. Patient education will occur throughout all components of CDT.
Effective management of swollen extremities starts with a comprehensive assessment of the patient. Understanding the true underlying cause of swelling, assessing their lower extremity vascular status (arterial and venous), and the patient’s goal will lead to proper interventions. Treating swelling and weepy extremities without adequate compression can progress inflammatory changes that lead to frequent infections, fibrosis of tissue, and damage to intact skin due to wetness (which will progress to lymphatic involvement). Once the lymphatic system is involved, the treatment must include all the components of CDT. Failure is imminent when treatment is only focused on treating the symptoms and not the underlying cause.
Click Here for a PDF Version of This Article
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Do you need more information on other topics on lymphedema? Use the “Index” list on the left side of this page and select the article you are interested in. You can also use the “Select Category” window on the right of this page and select the topic you are interested in. Once selected, a new page will load with a number of articles related to the topic you chose. Click on any headline of the articles and the entire article will load up for you to read.
Join Lymphedema Guru, a Facebook page solely dedicated to inform about all things related to lymphedema – news, support groups, treatment centers, and much more


Does fluid really get reabsorbed in the venous system or doe the new Starling principle at the microvascular level hold true where all fluid released into the interstitial space is picked up by lymphatic vessels?
thanks for wonderful article , that what I am dealing in every day my lymphedema practice