
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist.
Various surgical procedures for the treatment of lymphedema have been practiced for over a century and advancements in medical technologies have led to increased discussion of the role surgical treatment as an alternative or additional treatment option for a select group of patients affected by lymphedema. Recent research indicates that the surgical approach to treat lymphedema has beneficial effects for some patients; however, there is a broad consensus that surgical procedures do not eliminate the need of complete decongestive therapy (CDT) pre as well as post-operatively (1, 2), and should act as an adjunct to conservative treatment protocols.
 Any surgical approach to treat lymphedema should be reserved for those cases when conservative treatments have clearly been unsuccessful or when the achieved success of conservative measures can no longer be maintained (4).
Any surgical approach to treat lymphedema should be reserved for those cases when conservative treatments have clearly been unsuccessful or when the achieved success of conservative measures can no longer be maintained (4).
An important component to determine whether any surgical procedure for lymphedema is indicated is to weigh the potential benefit of the specific surgical procedure against the risks associated with it. Other considerations should include the individual medical needs and goals of the patient, and the medical expertise of the surgical team (5).
In general, surgical approaches can be classified as excisional techniques (debulking, liposuction), reconstructive techniques, and tissue transfer procedures.
This article covers reconstruction surgery and tissue transfer procedures for the treatment of lymphedema.
Lymphatic reconstructive procedures attempt to improve the rate of lymphatic return back to the blood circulation. Techniques include autologous transplant of functioning lymph vessels, lymph nodes or veins from other areas of the body into those areas affected by lymphedema, and the direct connection of lymph vessels and nodes to neighboring veins.
These procedures are mostly used in the earlier stages of lymphedema (before the occurrence of fibrotic and adipose tissues), in which the fluid component is predominantly responsible for the excess volume. Recent advances in micro surgical procedures and instruments, and improved imaging techniques led to continued progress in these procedures, and reductions in limb volume have been reported. However, no long-term studies are currently available on the effectiveness of these techniques, and more research is necessary to properly define indications for microsurgery.
Lympho-lymphatic anastomosis: This procedure involves the harvesting of healthy, functioning lymph vessels and transferring these vessels to the area affected by lymphedema, where they are sutured directly to the lymph vessels in the lymphedema-affected limb. The goal is to improve or restore lymphatic flow by creating a bridge bypassing the scarred or irradiated area. The healthy lymph vessels used in this procedure are usually taken from the inner thigh region, and there is a theoretical risk of inducing lymphedema at the donor site.
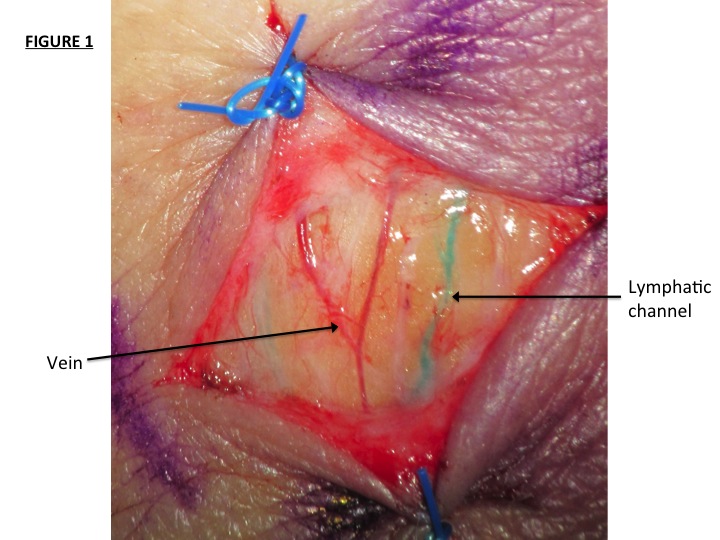 Lympho-venous anastomosis:
Lympho-venous anastomosis:
This procedure relies on the connection of lymphatic vessels in the area affected by lymphedema to small adjacent superficial veins (venules), allowing lymph fluid to directly drain into the venous system, thus bypassing areas of obstructed lymph flow. Better results tend to be achieved when numerous lymphatic-venous anastomoses are performed. No donor site is required for this procedure, which makes this procedure the least invasive with the lowest surgical risk.
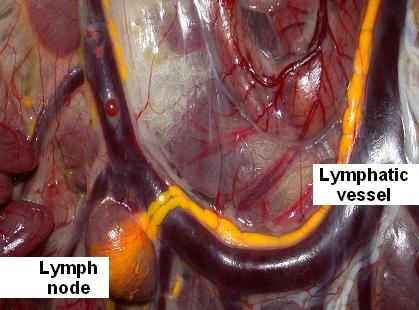 Vascularized lymph node transfer:
Vascularized lymph node transfer:
In this procedure autologous soft tissue containing lymph nodes with their arterial and venous blood vessels is harvested from a donor site (groin, chest wall or neck) and transplanted to the area affected by lymphedema. Here, the blood vessels of the donor tissue are connected to local blood vessels to re-establish blood supply to the transferred nodes. New lymphatic vessels are expected to sprout from the transplanted nodes and remaining lymph vessels are expected to re-grow, thus restoring lymphatic drainage and preventing formation of new scar tissue.
All surgical procedures are invasive, costly, involve significant risks, and the long-term results are not yet known. Conservative management of lymphedema with complete decongestive therapy is noninvasive, with minimal to no side effects for patients, shows excellent long-term results, and should always be the treatment of choice. CDT is considered the gold standard treatment for lymphedema and with properly applied treatment techniques and patient compliance is able to successfully manage lymphedema in the majority of patients (3).
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Join Lymphedema Guru, a Facebook page solely dedicated to inform about all things related to lymphedema – news, support groups, treatment centers, and much more
References:
1. Cormier JN, Rourke L, Crosby M, Chang D, Armer J. The surgical treatment of lymphedema: a systematic review of the contemporary literature (2004-2010). Ann.Surg.Oncol. 2012 Feb;19(2):642-51.
2. International Lymphedema Framework Position Document. Best Practice for the Management of Lymphoedema – 2nd Edition. Surgical Intervention. http://www.lympho.org/mod_turbolead/upload/file/Resources/Surgery%20-%20final.pdf (accessed January 28, 2016)
3. Cormier JN, Cromwell KD, Armer JM. Surgical Treatment of Lymphedema: A Review of the Literature and a Discussion of the Risks and Benefits of Surgical Treatment. Vol. 24 No. 2 – LymphLink Reprint
4. The Diagnosis and Treatment of Peripheral Lymphedema. 2013 Consensus Document of the International Society of Lymphology. Lymphology 46 (2013)1-11
5. Position Statement of the National Lymphedema Network on the Diagnosis and Treatment of Lymphedema. Updated Feb.2011
6. Granzow JW. The Current State of Surgery for Lymphedema. LymphLink Vol.28 No.4 3-6
7. Brorson H. Circumferential Suction-Assisted Lipectomy is the Only Surgical Procedure that Can Normalize a Large Chronic Non-Pitting Lymphedema. LymphLink Vol.28 No.4 7-9
8. Granzow JW, Soderberg JM, Kaji AH, Dauphine C. Review of Current Surgical Treatments for Lymphedema. Ann Surg Oncol DOI 10.1234/s10434-014-3518-8. Published online Feb 2014

